Speech Therapy After Stroke: When to Start


Dr. Krutika Bhadane
PT (Neuro), BPTh, MPTh (Neurosciences), 3+ years clinical
experience in neurological rehabilitation
Speech Therapy After Stroke: When to Start and What to Expect
Imagine sitting with your father the day after his stroke. He is awake, his eyes are open, he recognises you. But when he opens his mouth to say your name, nothing comes out the way it should. The words are there somewhere inside him. You can see the effort on his face. But they will not come. You hold his hand and try to smile, but inside, you are terrified. Will he ever speak normally again? Will he always be trapped like this?
This is one of the most painful moments a family can go through. And it happens more often than most people realise. Aphasia, dysarthria, or difficulty swallowing affects a large number of stroke survivors within hours of a brain attack. What many families do not know is that how quickly you act in the days that follow can shape everything that comes next.
Speech therapy after stroke is a structured rehabilitation process in which a trained Speech-Language Pathologist (SLP) helps a stroke survivor regain the ability to speak, understand language, read, write, and swallow safely.
This article explains when to start speech therapy, what to realistically expect during recovery, and covers angles that most articles overlook, including the bilingual reality in India, the role of swallowing therapy, and how modern technology is expanding what is possible even years after a stroke.
Why Does a Stroke Affect the Ability to Speak?
A stroke cuts off blood supply to part of the brain, damaging or destroying brain cells. When this damage affects the left hemisphere, specifically areas called Broca's area (responsible for producing speech) and Wernicke's area (responsible for understanding language), communication breaks down in very specific ways.
Most stroke survivors experience one or more of these three conditions:
- Aphasia: A language disorder that affects speaking, understanding, reading, and writing. It is the most common speech-related consequence of stroke.
- Dysarthria: A motor speech disorder where the muscles for speech become weak or uncoordinated. The person knows what they want to say but the words come out slurred or unclear.
- Apraxia of Speech: The brain loses the ability to sequence and coordinate the movements needed for speech, even though the muscles themselves work fine.
The Hidden Condition Most Articles Skip: Dysphagia

Here is what most websites do not tell you. Before speech therapy even begins in a clinical setting, the very first job of the SLP is not to work on speech. It is to assess swallowing.
According to research published by St. Mary's Health Care System, up to 64% of stroke patients experience difficulty swallowing, known as dysphagia. Research cited by Allied Services Integrated Healthputs this figure even higher, at 50 to 80% of stroke patients. If dysphagia goes unmanaged, the patient risks inhaling food or liquid into the lungs, which causes aspiration pneumonia, a potentially life-threatening infection.
SLPs assess swallowing within the first 24 hours of admission. Only once a safe diet consistency is established does the formal speech and language work begin.
Is your loved one newly discharged after a stroke? A swallowing and speech assessment is the critical first step.Book your initial evaluation at Apricot Care today. Schedule a Speech and Swallow Assessment
When Should Speech Therapy Start After a Stroke?
The short answer is: as soon as the patient is medically stable, which in most cases means within 24 to 48 hours of the stroke.
According to a 2025 review published in WCNR Congress, intensive speech therapy starting within 24 to 48 hours of stroke onset can significantly enhance long-term recovery outcomes.
Here is why the timing matters so much.
The Neuroplasticity Window: What the Brain Is Doing Right After a Stroke
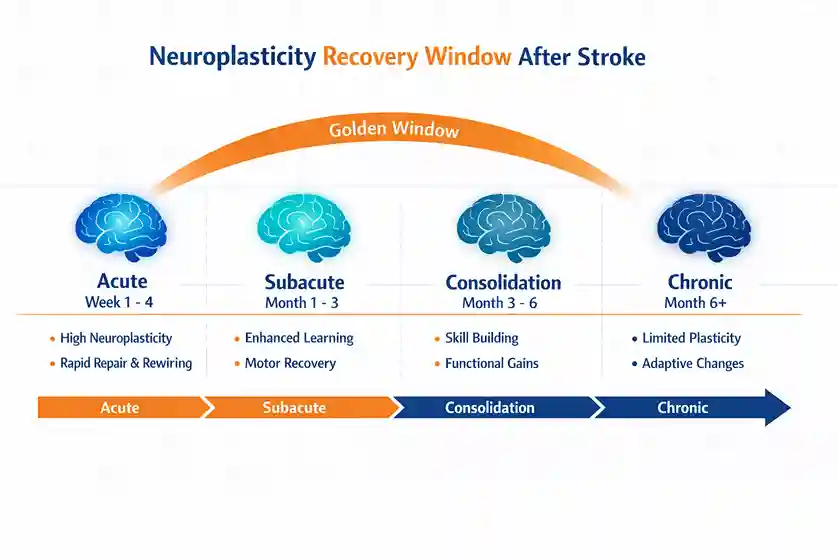
Your brain is not a fixed organ. After an injury like a stroke, healthy brain cells attempt to compensate for the ones that have been damaged by forming new connections and taking over lost functions. This process is called neuroplasticity, and according to a 2025 research review published in IJFMR, it underlies all recovery of speech and language after stroke. It is most active in the early weeks and months after injury.
Neuroplasticity is time-sensitive. The first three months after a stroke represent what clinicians call the golden window, where the brain is most capable of rewiring itself. This is when structured, intensive speech therapy produces the greatest gains. Waiting too long to start, whether due to lack of information, hospital discharge gaps, or the misconception that the patient needs to rest first, reduces this window.
Research from Taylor and Francis Online found that stroke survivors who received early clinical speech and language therapy in the first month had significantly better long-term speaking outcomes than those who did not. Among patients with moderate to severe initial aphasia, early structured therapy made a measurable and lasting difference.
What Most Families Are Told vs. What the Evidence Actually Says
Here is the gap between common advice and clinical reality:
| Topic | What Most Blogs Say | What Rarely Gets Said |
|---|---|---|
| Timing of therapy | Start early, ideally within 48 hours | The neuroplasticity window closes gradually; each week of delay reduces rewiring potential |
| What SLPs treat | Speech and language only | SLPs assess swallowing FIRST. Dysphagia affects 50 to 80% of stroke patients and causes aspiration pneumonia |
| Therapy intensity | Regular sessions are enough | 8 to 10 hours per week is the recommended minimum; intensity drives a 40% better outcome |
| Indian context | Not mentioned at all | Bilingual/multilingual aphasia is common in India and requires specialised SLPs |
| Recovery duration | 3 to 6 months | Meaningful gains are possible beyond 12 months with AI-assisted therapy |
| Emotional health | Brief mention | Depression affects 30 to 40% of aphasia patients and directly slows brain recovery |
What Does Speech Therapy Actually Look Like?
After an initial assessment using standardised tools like the Western Aphasia Battery, the SLP designs a personalised rehabilitation plan. This plan is built around the type of speech disorder, its severity, and the patient's overall cognitive state.
Evidence-Based Techniques Used in Clinical Practice
- Constraint-Induced Language Therapy (CILT): The patient is restricted from using gestures or writing and must communicate only verbally. This forces the brain to reactivate and strengthen its damaged language circuits.
- Melodic Intonation Therapy (MIT): Uses musical rhythm and singing to engage the right hemisphere of the brain in language production. Particularly effective for non-fluent aphasia where the patient can produce sounds but not words.
- Oral Motor Exercises: For dysarthria patients, these exercises strengthen the tongue, lips, jaw, and throat muscles to restore speech clarity.
- Swallowing Maneuvers: Techniques like the Mendelsohn maneuver, effortful swallow, and supraglottic swallow are used to improve swallowing coordination and reduce aspiration risk.
- TMS and tDCS (Brain Stimulation): Transcranial Magnetic Stimulation and transcranial Direct Current Stimulation are non-invasive tools used alongside speech therapy to modulate cortical excitability and enhance neuroplasticity. Research published in MDPI confirms their safety and emerging clinical benefit.
How Many Hours of Therapy Are Needed?
This is where most guides fall short. They say "regular therapy" without specifying what that means. But intensity matters enormously.
According to research cited by WCNR Congress, patients receiving intensive speech therapy of 3 to 5 hours daily show 40% better outcomes than those receiving standard care of 1 to 2 hours, 2 to 3 times per week. The American Speech-Language-Hearing Association recommends a minimum of 8 to 10 hours of direct therapy per week during the acute recovery phase.
Higher intensity therapy also produces significantly better functional communication, as confirmed by a meta-analysis published in Stroke journal (American Heart Association) The research showed that those receiving high-intensity SLT had significantly better outcomes on functional communication measures than those receiving low-intensity therapy.
Speech Recovery Milestones: A Realistic Timeline
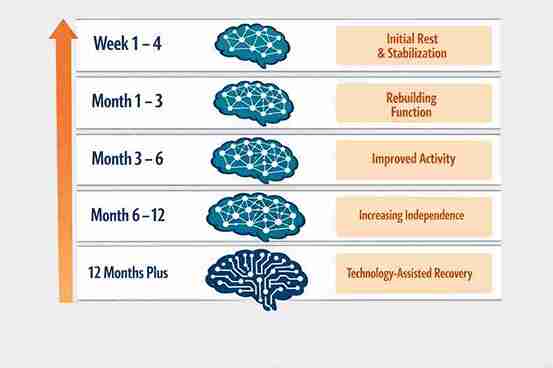
Families often ask: when will my loved one be back to normal? The honest answer is that recovery varies significantly from person to person. What matters is setting realistic expectations at each stage so that progress is recognised and motivation is maintained.
| Timeframe | What Happens in the Brain | What to Realistically Expect |
|---|---|---|
| Week 1 to 4 | Peak neuroplasticity window; brain starts forming new pathways | Swallowing safety is established first; basic yes/no responses, facial gestures |
| Month 1 to 3 | Rapid rewiring phase; damaged areas compensated by healthy regions | Word retrieval starts improving; short phrases become possible |
| Month 3 to 6 | Consolidation; newly formed pathways get reinforced through practice | Sentence construction begins; reading and writing exercises introduced |
| Month 6 to 12 | Plateau risk period if therapy stops; gains slow but remain possible | Structured intensive therapy prevents regression and deepens gains |
| 12+ Months | Chronic phase; brain retains some plasticity with right stimulation | AI-assisted therapy and telerehabilitation continue to drive meaningful recovery |
According to WCNR Congress 2025, approximately 60 to 70% of stroke survivors with aphasia show some degree of improvement within the first year. Younger patients under the age of 65 have better recovery outcomes overall, with 75% showing significant improvement compared to 55% in older patients. But the most important message here is this: recovery does not stop at six months. With the right therapy, meaningful gains remain possible well beyond the first year.
Recovery does not follow a single timeline. At Apricot Care, our SLPs in Pune build personalised therapy plans that adapt as your loved one progresses. about our stroke rehabilitation programme. Learn Explore Stroke Care at Apricot Care Pune
The India-Specific Reality Nobody Talks About
Most articles on speech therapy after stroke are written from a Western clinical context. But in India, the situation has unique complexities that matter enormously for recovery.
The Bilingual and Multilingual Challenge
Most Indians speak at least two languages fluently, and many speak three or four. When a stroke causes aphasia, it does not affect all languages equally. A patient who spoke Marathi, Hindi, and English before a stroke may lose fluency in one language faster than another, or may mix words from different languages involuntarily.
A landmark study on aphasia rehabilitation in India, published in Healthcare in February 2026, found that SLPs across the country reported significant challenges in managing bilingual and multilingual patients with aphasia. The same study stressed the need for developing rehabilitation materials and mobile apps specifically in Indian languages as an urgent priority.
This is not a minor clinical footnote. It means that a stroke patient in Pune who primarily thinks and communicates in Marathi needs an SLP who can assess and treat in Marathi, not just in English. This is a real and underserved gap in the Indian rehabilitation system.
The Urban-Rural Divide in Access to SLPs
Research from PMC India highlights that a majority of stroke survivors in India have limited or no access to rehabilitation services, as most trained SLPs are concentrated in cities like Pune, Mumbai, Delhi, and Bengaluru. Patients from smaller towns and rural areas often receive no formal speech therapy at all after discharge, relying entirely on family members with no clinical training.
This makes it critically important that urban rehabilitation centres like those offering stroke care in Pune not only deliver in-clinic therapy but also train family caregivers and offer telerehabilitation that can extend care beyond city limits.
The Role of Family Caregivers in Speech Recovery
Family involvement in speech therapy is not optional. It is clinically significant. Stroke survivors who receive consistent communication support at home recover faster and maintain gains for longer.
What Caregivers Should Do
- Speak at a normal pace and use short, simple sentences
- Give the patient time to respond without interrupting or filling in the words for them
- Use visual cues such as pointing to objects, pictures, or writing key words
- Practice daily home exercises recommended by the SLP for 15 to 30 minutes per day
- Celebrate small wins such as a new word or a clearer sentence, because emotional motivation drives neuroplasticity
What Caregivers Must Avoid
- Finishing the patient's sentences out of impatience or discomfort
- Speaking on behalf of the patient in all situations, removing their chance to try
- Showing visible frustration, sighing, or rushing communication moments
- Assuming the patient cannot understand because they cannot speak, as comprehension and speech are often separate functions
Technology Is Changing What Is Possible in 2025 and Beyond
One of the most exciting developments in speech therapy after stroke is the growing role of technology, both as a supplement to clinical sessions and as a standalone tool in the chronic recovery phase.
Telerehabilitation: As Good as In-Person for Most Patients
A 2025 review published in World Journal of Advanced Research and Reviews covering data from randomised controlled trials over the past decade concluded that telerehabilitation was either superior or equal to traditional in-person rehabilitation for post-stroke patients. This is particularly significant for multilingual patients in India who may not have access to a bilingual SLP locally but can access one online.
Telerehabilitation is not a second-class option. For many patients, it offers a bilingual therapist, more flexible session timing, and the ability to practice in the comfort of the home environment where real communication happens.
AI-Assisted Speech Therapy
A September 2025 systematic review in PMC found that AI-assisted digital therapy platforms can enhance aphasia rehabilitation by dynamically adjusting task difficulty, analysing patient performance in real time, and providing immediate feedback through speech recognition and natural language processing. The consistency of results across studies was described as remarkable, showing that AI tools can match traditional therapy for impairment-level gains while also offering far greater practice dosage between sessions.
Emotional Health and Speech Recovery: The Link Nobody Discusses Enough
Post-stroke depression is one of the most underaddressed factors in speech recovery. Research consistently shows that depression affects 30 to 40% of stroke survivors, and aphasia itself significantly increases this risk because the patient is suddenly isolated, unable to express thoughts, ask questions, or connect with their family in the way they once did.
Depression directly slows down neuroplasticity. A brain under chronic emotional distress does not rewire as efficiently as one in a positive, stimulated state. This is why psychological rehabilitation must run in parallel with speech therapy, not after it.
Family members should watch for signs of withdrawal, tearfulness, irritability, or resistance to therapy. These are not character flaws. They are clinical symptoms that respond well to counselling, peer group support, and a therapy environment where the patient feels safe to try and fail without judgment.
Speech recovery works best when it is part of a holistic plan. Our multidisciplinary team at Apricot Care integrates speech therapy, psychological support, nutritional guidance, and caregiver training, all under one roof. Explore our online therapy options too. Book an Online or In-Clinic Consultation Today
Key Takeaways
What you need to carry with you from this article:
- Speech therapy must begin within 24 to 48 hours of a stroke whenever the patient is medically stable
- The SLP's first priority is swallowing safety, not speech, because dysphagia affects up to 80% of stroke patients and carries serious medical risks
- The first three months are the golden window for neuroplasticity; therapy intensity during this period has a direct bearing on long-term outcomes
- 8 to 10 hours of direct therapy per week is the recommended minimum for the acute recovery phase
- In India, bilingual and multilingual aphasia is a real clinical challenge that requires SLPs trained in regional languages
- Recovery does not stop at six months or twelve months; AI-assisted therapy and telerehabilitation are opening new doors in the chronic phase
- Family caregivers are part of the therapy team, and how they communicate at home matters enormously
- Emotional health and speech recovery are linked; depression in stroke survivors slows brain healing and must be addressed alongside language rehabilitation
Speech therapy after a stroke is not just about getting words back. It is about giving a person back their voice, their relationships, their sense of self. No two recoveries look exactly the same. But the families who start early, stay consistent, and treat the whole person, not just the symptom, tend to see the most meaningful progress.
So here is the question to sit with today: If your loved one has recently had a stroke and has not yet been evaluated by a Speech-Language Pathologist, what is stopping you from making that call? Every day in the golden window is a day the brain is ready and waiting.